Turner Syndrome
This month, we’re featuring a cause of primary lymphedema called Turner syndrome. There will be a video series that follows with two interviews: one with a therapist (Jana) and one with a patient (Dorothy) who has Turner syndrome & lymphedema. Turner syndrome may be called:
- 45,X syndrome
- Bonnevie-Ullrich syndrome
- monosomy X
- Ullrich-Turner syndrome.1
The condition affects 1 out of every 2,000-4,000 live births.2 The condition is a genetic mutation of the X chromosome, a sex chromosome.
Biology Refresher
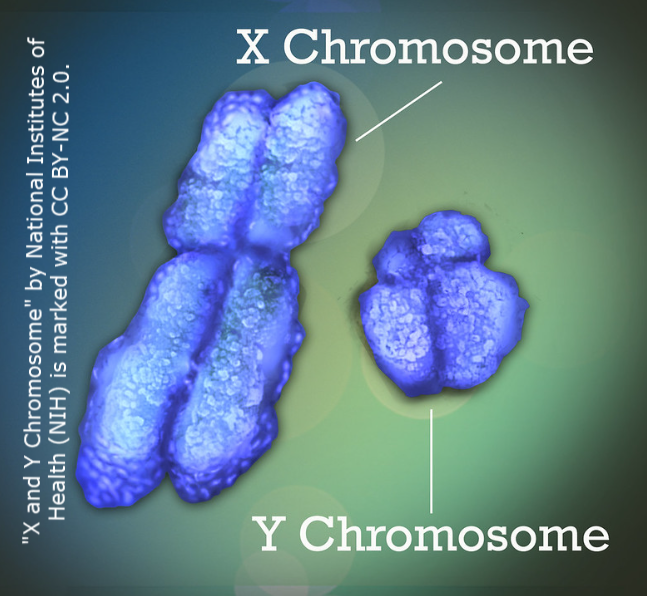
It may have been a while since biology class, so let’s refresh. A chromosome is a long chain of DNA that has part or all of the genes (genetic instructions) for an organism. People have 23 pair (or 46 chromosomes in all). Most are identical in men and women – except two:3 the X and Y sex chromosomes. Sex chromosomes determine the sex of an individual. Men have both an X and a Y. Women have two X chromosomes.
In Turner syndrome, part or all of the X chromosome is missing in women. (This condition only affects women though there is a similar but different version called Noonan’s syndrome that affects men.5) As a result, women do not develop normally.

The severity and extent of outcomes vary. Frequent symptoms include a short stature; short, webbed neck; low hairline; eyelids that turn downward; heart and kidney abnormalities; narrow palate; infertility; difficulty with spatial relationships; and, lymphedema (among others).
Primary vs Secondary Lymphedema
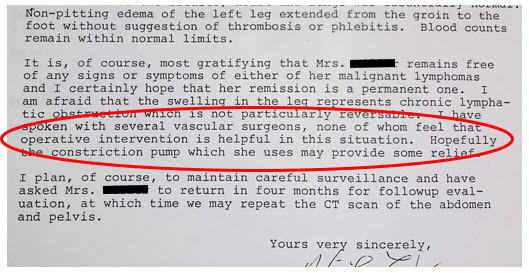
For our purposes, we’ll focus on lymphedema. The most common form of lymphedema is secondary. This means the lymphedema is due to a cause outside of itself such as: cancer, cancer treatment, venous insufficiency, obesity, infection, lipedema, surgeries, etc. The primary source results in structural damage to the lymphatic system. This structural damage causes impairment of fluid transportation back to the heart. Swelling results in the area damaged and may impact the entire extremity and trunk component that drains to that lymph node region. The swelling is chronic, inflammatory and will likely get worse over time.
In primary lymphedema, there is no cause outside of a congenital birth defect that results in abnormal lymphatic vessels and/or lymph node development. This abnormal development renders the lymphatic system in the affected area incompetent. As a result, swelling occurs which is chronic, inflammatory and often gets worse over time. Examples include Klippel-Trenaunay syndrome; Prader Willi; Milroy’s disease; Meige Disease; Noonan syndrome; Turner syndrome; Yellow Nail syndrome; Trisomy 13, 18, 21 and 22; and others.4
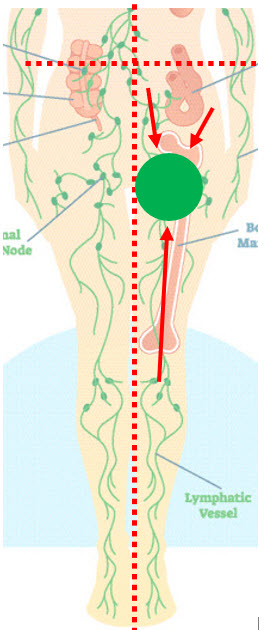
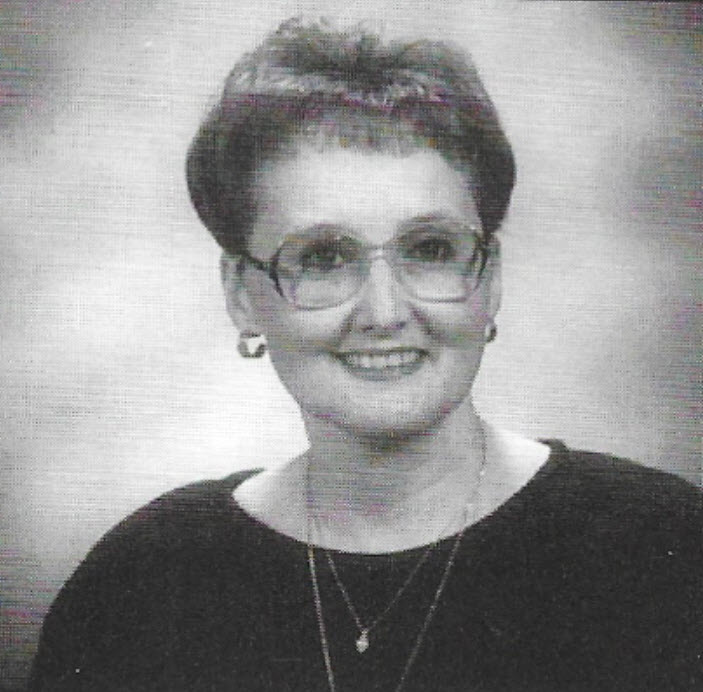
Because of the more severe complications of Turner syndrome that present as life-threatening, lymphedema is often an afterthought until a woman gets older and lymphedema progresses in severity (usually in the lower legs/feet). A common problem is finding shoes that fit as you’ll hear in the patient interview. Hands can be involved, too, but this may resolve as a child ages. Below are two images of Dorothy as a child.


References
1 Rare Diseases
https://rarediseases.org/rare-diseases/turner-syndrome/#:~:text=Consequently%2C%20in%20the%20past%2C%20Noonan,differences%20between%20the%20two%20disorders
2 Turner Syndrome Society
https://www.turnersyndrome.org/about-turnersyndrome
3 Medline
https://medlineplus.gov/genetics/understanding/basics/howmanychromosomes/#:~:text=In%20humans%2C%20each%20cell%20normally,in%20both%20males%20and%20females
4 Foldi, M, Foldi, E. (2006). Foldi’s Textbook of Lymphology (2nd ed.), p. 509-510. Germany: Urban and Fisher.
5 https://rarediseases.org/rare-diseases/noonan-syndrome/