There are many reasons for swelling—and not all of them are lymphedema. For example, did you know that atrial fibrillation (A-Fib) can sometimes lead to swelling? It can—but usually indirectly. A-Fib is one form of an irregular heart rhythm that can reduce how efficiently the heart pumps blood. In some people, especially those with underlying heart disease, this can contribute to fluid retention. In addition, some medications used to treat heart conditions can also cause swelling.
What is A-Fib
Atrial fibrillation (A-Fib) is the most common sustained abnormal heart rhythm. It begins in the heart’s upper chambers (the atria), most often in or near the left atrium around the openings of the pulmonary veins. Instead of contracting in a coordinated way, the atria quiver (fibrillate). This causes irregular electrical signals to reach the lower chambers (the ventricles), resulting in an irregular—and sometimes rapid—heartbeat.
Common symptoms include:
- Swelling
- Heart palpitations
- Fatigue
- Shortness of breath
- Dizziness
- Reduced exercise tolerance
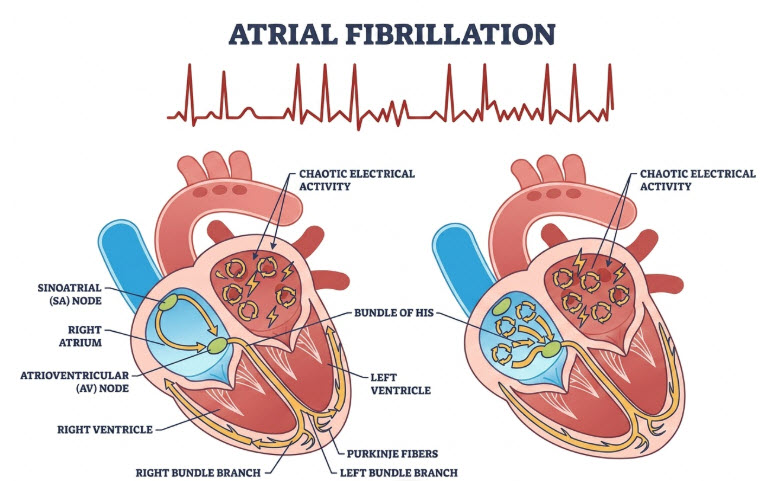
The abnormal electrical activity most commonly starts in or near the left atrium, often around the openings of the pulmonary veins.
How Swelling Can Occur
While most people never get swelling, fluid retention can occur for several reasons:
- Reduced pumping efficiency. During A-Fib, the atria don’t squeeze effectively. This can reduce how efficiently the heart fills and pumps blood, especially if the heart is already weakened.
- Heart failure can develop or worsen. If A-Fib is very fast or persists for a long time, the heart muscle can become less effective. When the heart can’t pump blood efficiently, fluid can back up in the body.
- Fluid backs up in the veins. When blood backs up, pressure in the veins increases. Fluid leaks from the blood vessels into surrounding tissues, causing edema (swelling).
Where Swelling is Seen
If the right side of the heart is affected—or if there is heart failure overall—fluid commonly collects in the legs, ankles, and feet. If the left side of the heart is affected, fluid is more likely to build up in the lungs, leading to shortness of breath rather than noticeable leg swelling.
This patient had leg & ankle swelling due to A-Fib and heart failure. They admitted to the hospital and had 12 pounds of “water weight” removed.


A few months later, swelling had reoccurred, but most resolved with medication change(s).
Who is most likely to develop swelling?
Swelling is more likely when AFib occurs along with:
- Heart failure
- Long-standing high blood pressure
- Heart valve disease
- Kidney disease
- Certain medications
For example, calcium channel blockers such as diltiazem (Cardizem) and verapamil can cause swelling of the feet and ankles. These medications relax blood vessels, which can allow more fluid to move from the bloodstream into surrounding tissues. This type of swelling is a medication side effect and is different from swelling caused by heart failure.













