Last month we noted there are several differences among pumps. And not all pumps are appropriate for all conditions. When it comes to lymphedema, the wrong pump has potential to do more harm than good. This month, we’re picking up with the types of compression pumps available.
Types of Compression Pumps (continued)
2. Non-Pneumatic Pumps – Non-pneumatic compression pumps use mechanical forces (rather than air) to apply compression. For example, Koya Medical (Dayspring device) uses shape-memory alloy springs that generate compression when activated by electrical current, causing the alloys to contract. This creates mechanical compression without air. These systems typically consist of a sleeve placed on a limb, and compression is delivered in a sequential or gradient pattern. Because they are lightweight, battery-powered, and allow mobility, users can often move or walk during treatment. (This is unique for lymphedema.) They are also generally quieter than pneumatic systems. (For those located in Dallas, Tx, Koya Medical relocated to the state in 2025.)
Common Uses:
- Management of chronic lymphedema
- Supporting lymphatic drainage in active patients
- Enhancing treatment adherence through mobility
Examples of Devices:
- Dayspring by Koya Medical
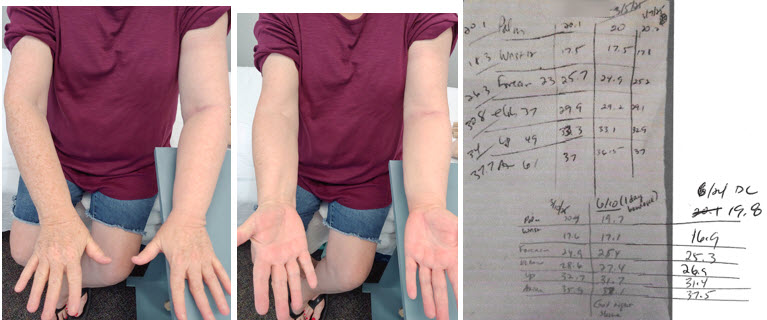
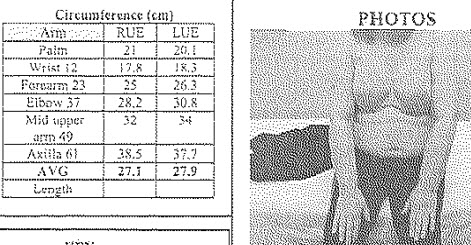
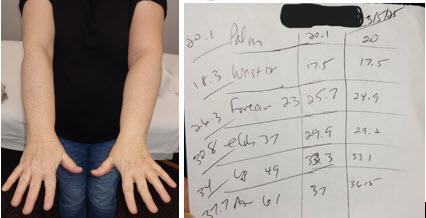
It’s important to note: Because they are lighter, less bulky and allow mobility, compliance may be improved. However, one downside from a therapist’s perspective is the sleeve doesn’t cover the hand (or the foot if on the leg). The concern is the potential to contribute to swelling in the hand and foot. Koya Medical believes that hand swelling is unlikely as they provide a mild compression glove and people are meant to be active, so a person is using their hand muscles to help reduce swelling. Another downside is the pump doesn’t first decongest the trunk as we do in manual lymph drainage lymphedema treatment. This is important in pure lymphedema as the swelling involves a quadrant of the trunk due to the drainage path of the lymph system. So, a patient may need to be taught how to first open the lymph drainage path and initiate drainage if using this pump, etc.1

Well Pump – Public Domain (Pixabay)
Are Pumps Necessary for Lymphedema?
Many people (especially pump manufacturers & distributors) won’t agree, but in my experience treating patients with lymphedema, pumps are generally not needed. In fact, Foldi’s Textbook of Lymphology doesn’t recommend them. However, compression pumps have advanced since their writing. The National Lymphedema Network (NLN) recognizes this, but the NLN still considers a pump to be an adjunct to therapy, not a standalone or a necessary component to treatment.1,2
I would agree & have a few reservations about pumps in general:
- Insurance may pay several thousand dollars for one (as much as $8,000 in some cases – or more) but patients grow tired of using them. Patient complaints include:
- pump hoses are heavy & hard to put on or take off (elderly may not have the strength)
- the daily pumping schedule recommended (sometimes twice a day) is too time-consuming
- doesn’t always seem to help or the improvement doesn’t last without using compression garments
- Patients are frequently not informed about the contraindications or don’t know when they should stop using a pump
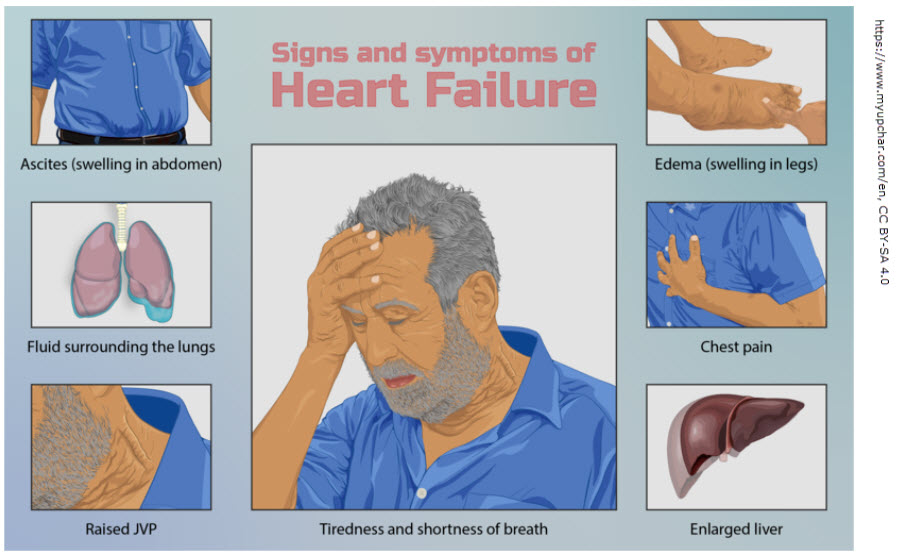
- Frequent pump use may worsen heart or kidney disease as it moves more fluid through the body & increases the load these organs must process. Too often, this isn’t well-monitored. At a minimum, people should monitor weight & blood pressure regularly in cases of “compensated” heart or kidney disease (as well as taking note of how they feel after pump use).
What are the best pumps for lymphedema?
Assuming you, your therapist & doctor have decided a pump would be beneficial for you, what are the best compression pumps for lymphedema? If dealing with pure lymphedema, first, ensure there is a trunk component like a vest or shorts. If there isn’t, ensure you’ve been taught how to decongest before pumping & how to clear after pumping. Second, ensure there are several chambers which pump proximally (at the root of the extremity) & works outward to decongest before pumping distal to proximal. For example, in right arm lymphedema due to breast cancer, be sure the pump begins pumping to decongest nearer the axilla & works outward toward your hand slowly, in segments, before pumping from the hand up to the axilla. Below are a list of potential manufacturers, but be sure the model chosen fits the recommendation: advanced, programmable, sequentially gradient compression (pneumatic or not). (Note this rules out most inexpensive, Amazon-purchased pumps.)
- Bio Compression Systems
- Lympha Press
- Airos Medical
- Tactile Medical
Runner-up: Koya Medical
References
1 Foldi, M, Foldi, E. (2006). Foldi’s Textbook of Lymphology (2nd ed.), p. 282. Germany: Urban and Fisher.
2 https://lymphnet.org/page/position-papers