One of the more popular posts I’ve written is about contraindications to treatment (time when treatment should not be done). Lymphedema treatment includes manual lymph drainage (MLD), multi-layer short-stretch bandaging, skin care and exercise. Both MLD & bandaging have specific precautions.1
General Precautions
The general precautions for MLD include:
– Active infection (caused by pathogens)
– Untreated cardiac failure
– Renal failure
There’s a relative contraindication for MLD:
– Malignant lymphedema (active cancer is causing the swelling)
Specific Precautions
But there are also specific precautions for MLD depending on where it is performed on the body. A sequence for MLD typically starts at the neck where the fluid drains. It doesn’t matter if swelling is in the legs, arms, head or elsewhere. But not all people will be appropriate for a neck sequence due to specific contraindications. For example, if someone has a cardiac arrhythmia related to an atrioventricular block or “AV-block” (referring to a block of the AV node in the heart’s electrical system). Doing a neck sequence could potentially stimulate the vagus nerve and cause cardiac arrest.

Understanding General Precautions (Active Infection)
So why are the general precautions a concern? In the case of an active infection caused by a pathogen (like bacteria in a cellulitis infection), performing MLD may cause the infection to spread. Fascinatingly, even though arterial & lymphatic flow increases during inflammation, in local inflammation, lymph vessels near the site of infection constrict. Thisprevents bacteria from escaping and entering the rest of the circulation. In performing MLD, this spasm could be relaxed, allowing normal flow to resume. The bacteria might then be allowed to move into the rest of the body & the infection could become systemic (i.e. sepsis).
(Untreated Heart Failure)
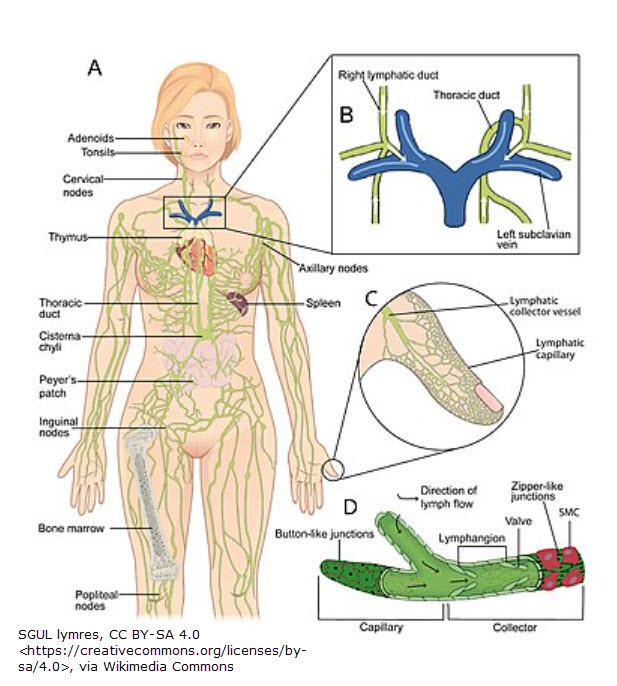
In the case of untreated heart failure, the concern is increasing pressure. The pressure in the veins returning blood to the heart near each collar bone (clavicle) is usually low. This is where lymphatic fluid returns to the body’s blood circulation. In untreated heart failure, the pressure is increased in these veins. Stimulating lymph flow with MLD would only add more fluid to a congested area and further increase the pressure. This can contribute to heart damage.
(Kidney Failure)
In the case of kidney failure, there is swelling in the body (often the lower part of the body). MLD would increase the amount of fluid returning to the heart and subsequently to the kidneys, increasing the fluid they must filter. This could overtax them. But the main reason MLD is not performed is because it would be of no use (if swelling being treated is due to kidney failure). That’s because kidney-caused swelling is edema, not lymphedema. The lymph vessels are already working as hard as they can to help get rid of the excess fluid. MLD speeds up lymphatic flow but beyond its normal high-working speed.
(Active Cancer)
In the case of cancer, MLD is a relative precaution. Meaning, there’s some room for discernment. The primary reason for avoiding MLD in the case of cancer is the potential to spread the cancer cells. (Cancer spreads through one of two ways: blood or lymph flow.) However, according to Foldi, molecular biology showed metastasis formation is an active process controlled by the cancer cells themselves. For example, cancer cells secrete a protein called vascular endothelial growth factor C (VEGF-C). 2 This is responsible for creating new lymphatic vessels within and around a tumor from existing ones (lymphangiogenesis). Nonetheless, many therapists prefer to avoid the area of the tumor to avoid any potential accusation of / or potential of hastening cancer cell transportation.
It’s also important to know if a patient is receiving adequate cancer treatment and that the cancer is responding. One note: Some suggest avoiding MLD for 2-3 days after chemo to allow the drug(s) to remain in the body and do their job. Others suggest proceeding with MLD to help distribute the chemo throughout the body and to use gloves to prevent transmission of chemo through the skin to the therapist. I would tend to side with the former group (avoid MLD – at least in the area of the body directly affected by the tumor1). But it’s important to check with the oncologist before providing any treatment.
References
1 Foldi, M, Foldi, E. (2006). Foldi’s Textbook of Lymphology (2nd ed.), p. 275-276. Germany: Urban and Fisher. Foldi, M., & Foldi, E. (2012). Foldi’s Textbook of Lymphology (3rd ed.). Urban and Fisher.
2 Yan, H., Zhang, C., Wang, Z. et al. CD146 is required for VEGF-C-induced lymphatic sprouting during lymphangiogenesis. Sci Rep 7, 7442 (2017). https://doi.org/10.1038/s41598-017-06637-7