Staying informed about insurance rule changes related to the Lymphedema Treatment Act is essential for both patients and providers. Since the law’s implementation under Centers for Medicare & Medicaid Services Medicare Part B in 2024, updates to coverage guidelines, billing requirements, and documentation standards continue to evolve. Keeping up with these changes helps ensure patients receive the compression garments and supplies they need without unnecessary delays or coverage issues.
Lymphedema Treatment Act Summary
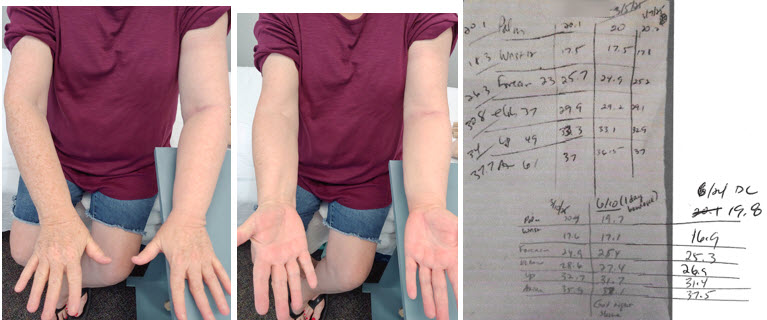
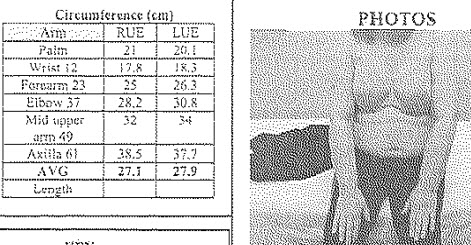
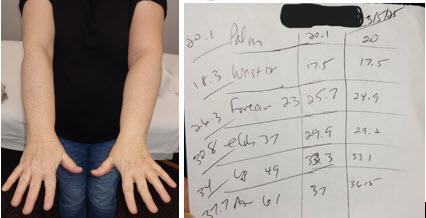
For years, individuals living with lymphedema struggled to get Medicare coverage for compression garments and related supplies. Sometimes patients couldn’t afford to buy the necessary items to maintain volume loss in therapy, or they had to substitute with substandard items. Lymphedema Treatment Act (LTA) changed that.

The Lymphedema Treatment Act is a federal law that requires Medicare to cover compression garments and other lymphedema treatment supplies when they are prescribed by a physician for a patient diagnosed with lymphedema and documentation supports medical necessity.
A new category for lymphedema compression was created (instead of being classified as standard “durable medical equipment”). The law was passed by Congress on December 23, 2022 (as part of the Consolidated Appropriations Act of 2023) after more than a decade of patient advocacy and legislative effort. It went into effect January 1, 2024.
What’s Covered
Medicare Part B now covers off-the-shelf and custom-fitted compression garments, wraps, bandaging systems, and accessories used for treating lymphedema — including donning and doffing aids, padding, fillers, linings, and zippers.1,2
- Coverage includes frequency guidelines such as three daytime garments every six months and two nighttime garments every two years per affected body part.
- Coverage only applies to items prescribed for diagnosed lymphedema and requires adherence to Medicare’s documentation and billing rules.
A person must have a diagnosis of:
- I89.0 – Lymphedema, not elsewhere classified
- I97.2 – Postmastectomy lymphedema syndrome
- I97.89 – Other postprocedural complications and disorders of the circulatory system, not elsewhere classified
- Q82.0 – Hereditary lymphedema
Where to Get Compression Garments
You must purchase compression from a Medicare supplier. Therapists & therapy clinics can be suppliers, but they must go through the credentialing process as a Durable Medical Equipment supplier (i.e. have a state DME license, additional DME insurance, etc.) & meet supplier standards. (Lymphedema Therapy Source is a DME supplier for our patients.)
Staying Informed
There are changes and updates to this federal law. Below are a couple of good sites to follow to stay informed about those changes:
- Compression Alliance Video on Billing Updates: US Medical Compression Alliance
- Lymphedema Advocacy Group: https://lymphedemaadvocacygroup.org/

The U.S. Medical Compression Alliance (USMCA) is an industry coalition of medical device manufacturers that focuses on improving care and access to medical compression therapy for patients with venous and lymphatic diseases (such as lymphedema and chronic venous insufficiency).
Conclusion
The Lymphedema Treatment Act didn’t just change a policy — it changed lives. It means that patients can now get the compression supplies they need without prohibitive out-of-pocket costs. And because Medicare often sets the standard that private insurers follow, this law has the potential to widen coverage across many plans, expanding access even beyond Medicare beneficiaries.
References
1 https://lymphedemaadvocacygroup.org/lta-coverage-rules
2 https://www.cgsmedicare.com/jc/pubs/news/2023/12/cope147943.html