The last two months we learned the brain has lymphatics in the outer meningeal layer (which is just beneath the skull). We also learned an accumulation of waste in the CNS is the likely cause of neurological pathology.
The Disease Process
Specifically, two types of waste accumulate in the CNS during this neuropathology:
- amyloid beta peptide – a metabolic waste product in the brain created during neuronal activity &
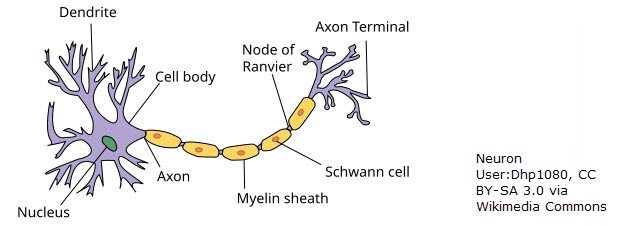
- phosphorylated tau protein – tau protein that has become highly phosphorylated & insoluble. That is to say, when multiple phosphate groups are added to its structure, tau can detach from microtubules (the “highways” within neurons) & cause neurofibrillary tangles that block the neuron transport system. This causes cells to die.

To summarize, the accumulation of these waste products leads to inflammation, cell death & the symptoms seen in neurological diseases like Alzheimer’s (a form of dementia), multiple sclerosis, Parkinson’s & traumatic brain injury among others.1 The reason for this waste buildup is a disruption in drainage of fluid from the CNS. How does fluid drain from the CNS?
CNS fluid drainage
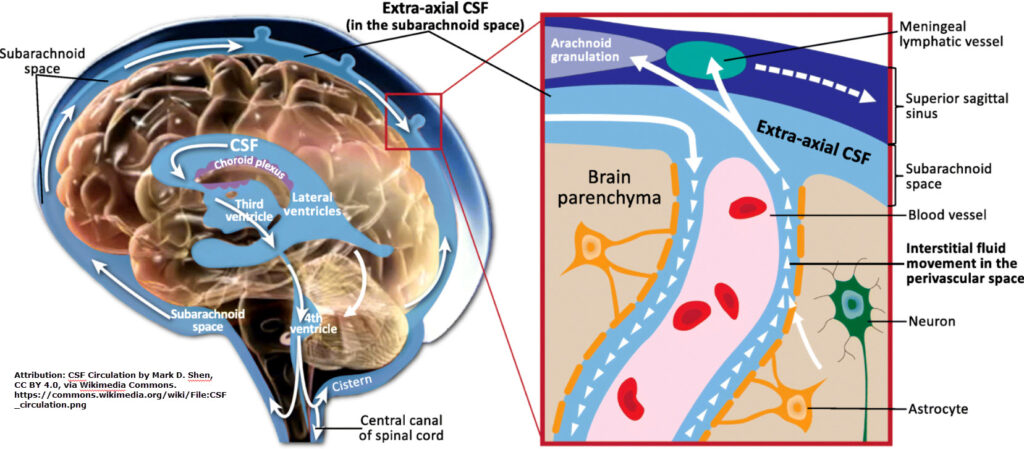
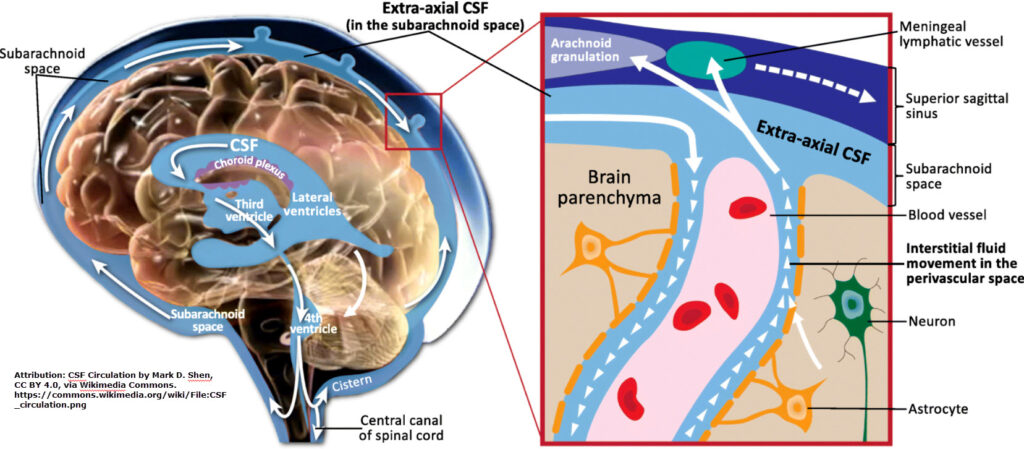
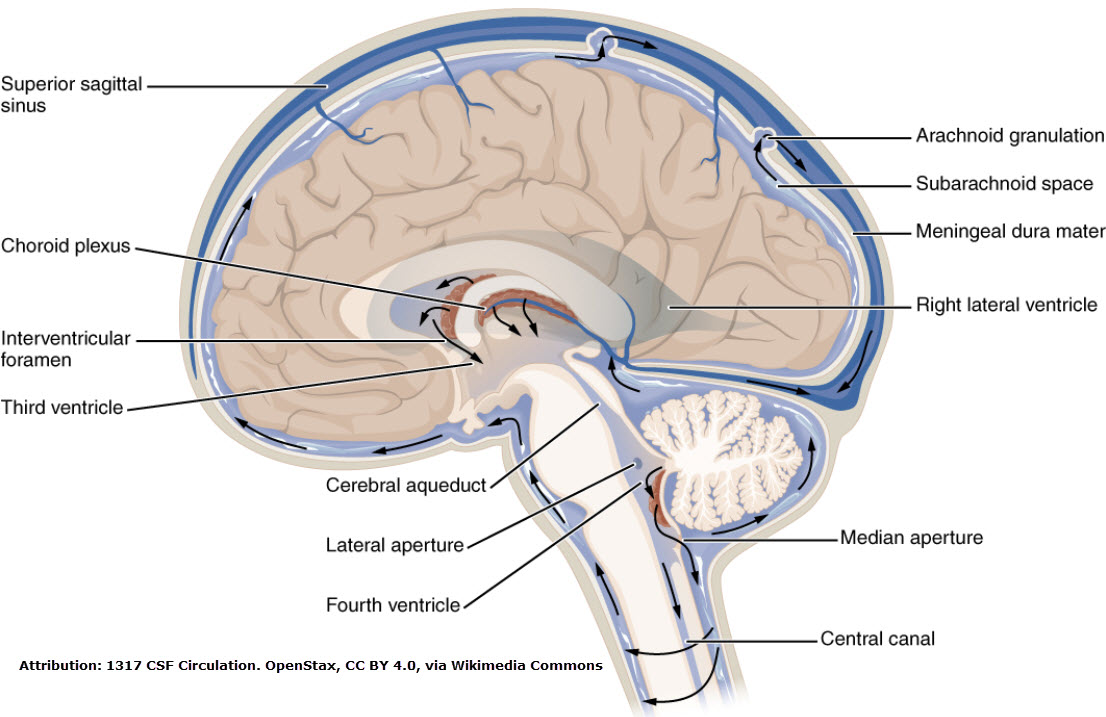
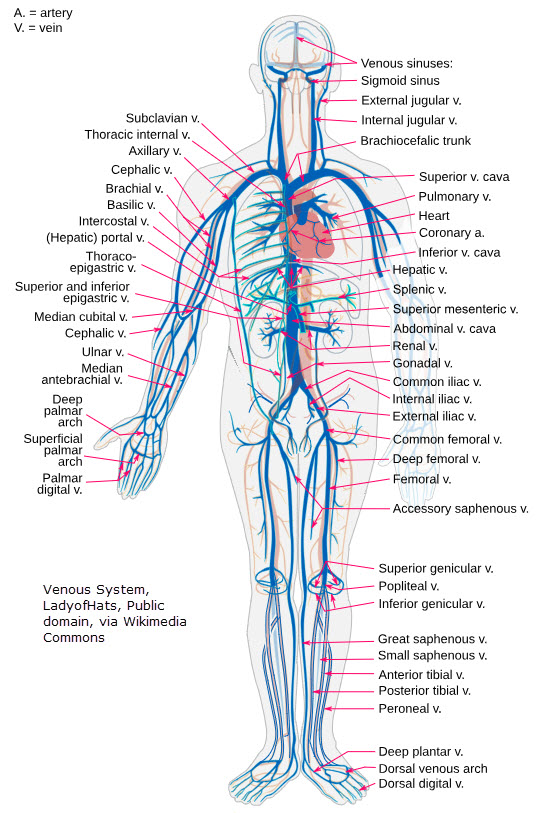
Fluid drains from the central nervous system through pathways similar to the rest of the body: veins & lymphatic pathways.2 The brain (cerebrum, cerebellum & brain stem) drain to the arachnoid (middle meningeal layer) & then to the dural venous sinus before emptying into the internal jugular veins.
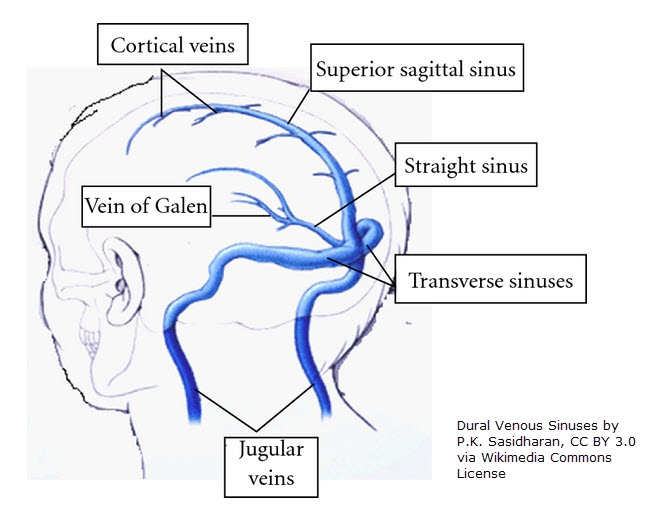
The dural venous sinuses are formed by the outer dura mater when it separates to form two layers within the dura mater (one that lines the skull & one that continues around brain tissue).
Interesting fact: In Latin, “dura” means tough & “mater” means mother. Your dura mater is a tough mother!
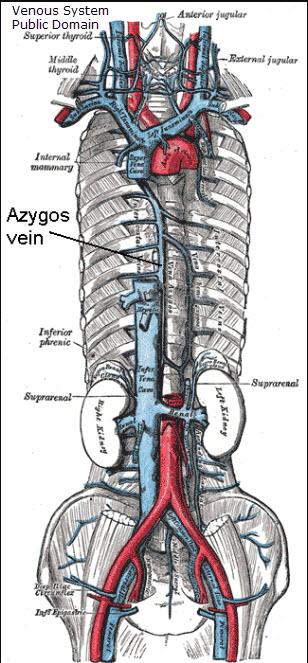
The spinal cord drains to a network of veins along the spinal cord called the vertebral plexuses. This pathway is a bit more complicated.5,6 For example, the cervical (neck) portion drains to the vertebral veins before emptying to the brachiocephalic veins, the subclavian veins, the superior vena cava & the heart.3 Other spinal cord sections drain differently. But all blood eventually drains to either the superior vena cava or the inferior vena cava before entering the heart.
Lymph fluid drainage
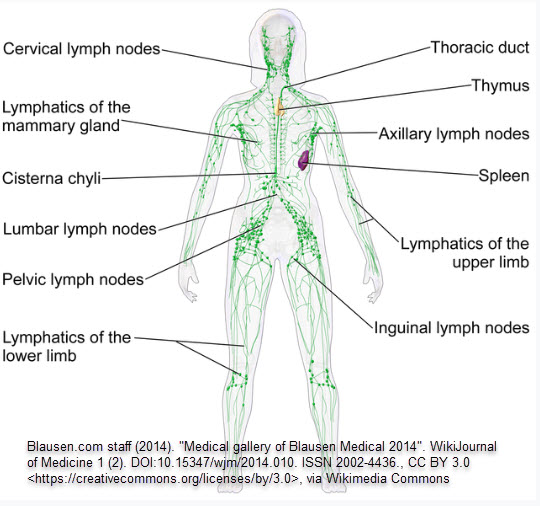
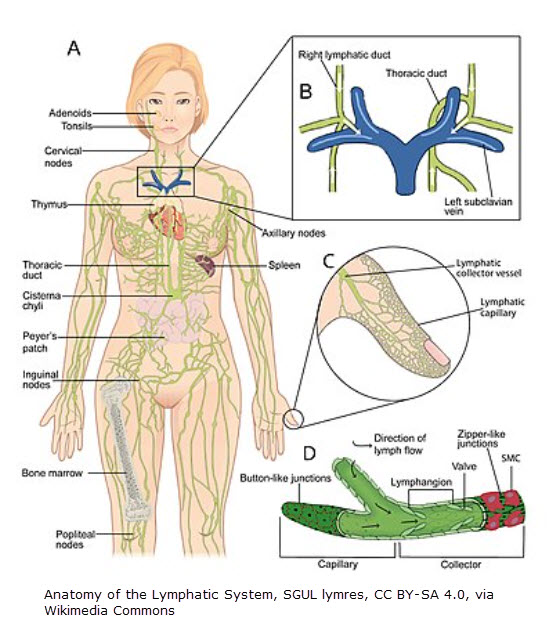
In the last couple of months, we also learned that CNS fluid mixes with interstitial fluid before draining to lymph vessels in the outer meningeal layer (the dura mater). From there (focusing on the brain), fluid drains to the cervical lymph nodes in the neck.
Image depicting lymphatic drainage from the head & neck as it returns to the heart.
What CNS drainage & lymphedema have in common
As we’ve already learned, when CNS drainage is disrupted, it causes congestion & the accumulation of amyloid beta peptide & phosphorylated tau protein. This results in inflammation, cell death & the symptoms associated with neurological diseases.
A similar process happens in lymphedema. When lymphatic drainage is disrupted, it causes congestion & the accumulation of the lymphatic load (protein, in particular). This results in inflammation, tissue remodeling & symptoms (swelling, tissue hardening, skin changes, etc.) associated with lymphedema. Conservative treatment is complete decongestive therapy (CDT). One of the components of CDT is manual lymph drainage (MLD). And herein lies a key to the answer of our blog heading: Can MLD Slow Cognitive Decline?
Professor Michael Foldi
A medical doctor, Professor Foldi & his wife (also a physician) have spent years researching, collaborating, teaching, & treating patients with lymphedema. In 1966, Professor Foldi said, “The potential role of the lymphatic system should never be disregarded in any disease of the central nervous system.”7 In the chapter on lymphostatic diseases in the Foldi textbook, Wolf Lüdemann (physician) did a study in 2004 showing the positive influence of MLD on intracranial pressure in severe traumatic brain injury.8 A 2016 article showed cervical & cranial MLD improved intracranial pressure as well as did a 2023 study.9,10
How MLD could impact CNS drainage
Deeper lymph vessels called collectors have components called lymphangions. Lymphangions have a proximal & distal valve as well as muscle that moves lymph through the collectors. “During the systole of the lymphangion, the proximal valve is open and the distal valve is closed. The lymph is pumped into the next lymphangion, which is in its diastole at that moment. “A lymphangion responds to an increased load like the heart.”12 In fact, lymphangions are sometimes referred to “mini-hearts.” When at rest, the lymph flow (per unit of time) is low. But when lymph flow increases, then the amount of lymph entering a lymphangion also increases. This causes the wall of the lymphangion to be stretched & lymph fluid to be transported. “Stretching the lymphangion wall from the outside through manual lymph drainage has the same effect!”13
Improving neurological conditions like dementia
In closing, MLD impacts the flow of lymphatic fluid. When there is congestion as can be seen in the CNS in neurological conditions like dementia, MLD may very well reduce this congestion by stimulating lymph drainage. In fact, Foldi’s Textbook states, “Fostering the lymphatic drainage of β-amyloid in older persons could prevent its accumulation in the brain, could sustain homeostasis, and could represent a treatment strategy to prevent the decline of mental faculties in Alzheimer’s disease.”11 I would caution that not all MLD is the same. Just because a technique is called “MLD” doesn’t mean it is. See also Guenter Klose’s presentation for LERN.
The original form of MLD (as developed by Dr. Vodder & taught by the Foldi’s) is a two-way stretch of the skin. There are specific characteristics of proper MLD in addition to being a two-way stretch of the skin. These characteristics include being slow (1 second per repetition) & rhythmical among other characteristics.
To learn more about other potential ways to slow cognitive decline, check out this podcast with Dr. Heather Sandison. To learn how microplastics could be contributing to inflammation, check out this interview. You know what else could benefit from MLD? Nerve inflammation. Find out how trigeminal neuralgia & Bell’s Palsy could be improved with MLD next month.
References
1 Bakker EN, Bacskai BJ, Arbel-Ornath M, et al. Lymphatic Clearance of the Brain: Perivascular, Paravascular and Significance for Neurodegenerative Diseases. Cell Mol Neurobiol. 2016;36(2):181-194. doi:10.1007/s10571-015-0273-8; link https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4844641/)
2 Adigun OO, Al-Dhahir MA. Anatomy, Head and Neck: Cerebrospinal Fluid. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459286/
3 https://www.kenhub.com/en/library/anatomy/vertebral-vein
4 https://www.youtube.com/watch?v=WTu31680f6s
5 https://www.physio-pedia.com/Spinal_Cord_Anatomy
6 Green K, Reddy V, Hogg JP. Neuroanatomy, Spinal Cord Veins. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. (https://www.ncbi.nlm.nih.gov/books/NBK542182/)
7 Földi, Michael; Földi, Ethel; Strößenreuther, Cornelia; Kubik, Stefan. Földi’s Textbook of Lymphology: for Physicians and Lymphedema Therapists (German Edition) (p. 715). Elsevier Health Sciences. Kindle Edition.
8 Földi, Michael; Földi, Ethel; Strößenreuther, Cornelia; Kubik, Stefan. Földi’s Textbook of Lymphology: for Physicians and Lymphedema Therapists (German Edition) (p. 774). Elsevier Health Sciences. Kindle Edition.
9 Roth C, Stitz H, Roth C, Ferbert A, Deinsberger W, Pahl R, Engel H, Kleffmann J. Craniocervical manual lymphatic drainage and its impact on intracranial pressure – a pilot study. Eur J Neurol. 2016 Sep;23(9):1441-6. doi: 10.1111/ene.13055. Epub 2016 May 30. PMID: 27238738.
10 Esparza WD, Aladro-Gonzalvo AR, Ruíz-Hontangas A, Celi D, Aguirre MB. The Effect of Craniofacial Manual Lymphatic Drainage after Moderate Traumatic Brain Injury. Healthcare (Basel). 2023;11(10):1474. Published 2023 May 18. doi:10.3390/healthcare11101474
11 Földi, Michael; Földi, Ethel; Strößenreuther, Cornelia; Kubik, Stefan. Földi’s Textbook of Lymphology: for Physicians and Lymphedema Therapists (German Edition) (pp. 717-718). Elsevier Health Sciences. Kindle Edition.
12 Földi, Michael; Földi, Ethel; Strößenreuther, Cornelia; Kubik, Stefan. Földi’s Textbook of Lymphology: for Physicians and Lymphedema Therapists (German Edition) (p. 450). Elsevier Health Sciences. Kindle Edition.
13 Földi, Michael; Földi, Ethel; Strößenreuther, Cornelia; Kubik, Stefan. Földi’s Textbook of Lymphology: for Physicians and Lymphedema Therapists (German Edition) (p. 450). Elsevier Health Sciences. Kindle Edition.