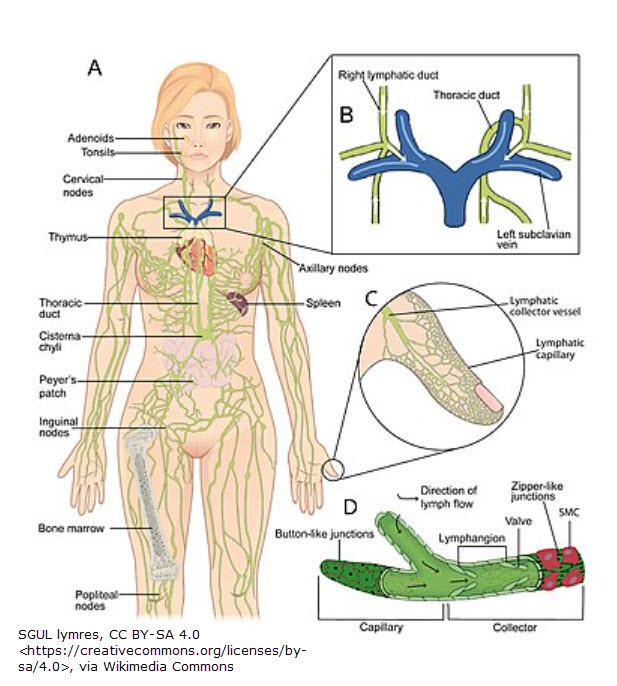
This post will wrap up (for now) Medicare’s recent passage of the Lymphedema Treatment Act (LTA) requiring coverage of lymphedema compression & supplies. (Included will be pictures of a few examples.) One concern I cited last month was the competency of the typical DME supplier to fit compression garments. I will expand on that in this post.
Bill Coverage summary
You can read last month’s post for a more comprehensive overview of what will be covered in the LTA. You can find the final Medicare rule here.
Swell spot (by JoViPak) – use to break up fibrosis or fluid pocketing on the chest wall & under the armpit typically related to breast cancer & mastectomy.
In short, compression garments (readymade or custom) & treatment supplies will be covered. Additionally, accessories like donning or doffing aids will be included in the coverage (items which help you put compression on or take it off).5 These will be covered at 80% (with 20% being your responsibility depending on what coinsurance you have). Garments are subject to the Medicare deductible.
Regarding frequency, as noted on p. 58 & 60 of the above final rule link:
- Medicare has increased the frequency limitations to (3) sets of daytime compression garments every 6 months & (2) nighttime garments every two years.
- Medicare doesn’t propose a specific frequency for bandaging systems & supplies (including accessories). The DME company will have to determine what is “medically necessary.”
Swell spot for the neck such as may be needed after head/neck cancer.

DME supplier requirements
Anyone providing DME-covered items must be a licensed DME supplier. That means a company must be enrolled with Medicare as a DME supplier & meet supplier standard requirements. There are several steps (& expense) to this process.
What is not highlighted is how important the knowledge & competency of a fitter is. A fitter should have a broad understanding of lymphedema & related pathology. Under this heading I would include an understanding & awareness of the following (non-comprehensive) list:
- causes & complications of lymphedema
- the disease process of the above lymphedema causes
- for example, lipedema compression tolerance in stage 1 vs stage 3
- for example, cancer precautions
- complications of common comorbidities such as
- weakness due to arthritis
- restrictions due to arterial disease
- restrictions due to fragile, thinning skin
- limited mobility, back precautions & safety donning/doffing compression (or modification of tools)
- edema-causes of swelling (like heart failure or venous reflux) which may not tolerate circular-knit hose
- adaptive devices for assisting donning/doffing compression
- recognizing & knowing how to address pressure spots caused by garments
- textile properties & how they affect tissue containment
- for example, gradient pressure or working pressure vs resting pressure

Farrow Velcro sleeve & readymade glove (readymade means it’s not custom).
DME supplier recommendations
While standard DME companies can address basic DME items like walkers, canes, wheelchairs, etc., fitting compression garments requires a more nuanced knowledge. Ideally, the fitter would also be an experienced lymphedema-certified therapist. An experienced therapist will have a working knowledge of lymphedema, comorbidities, problems with donning/doffing & creative solutions. They will have an idea of long-term outcomes associated with particular garments & lymphedema or related conditions. A therapist would also be an ideal person to educate patients on topics listed in the prior section.
But just because a therapist has experience treating lymphedema doesn’t mean they have experience fitting patients with compression. For example, fitting custom garments is a developed skill, & measuring technique can vary between manufacturers. In addition, an experienced lymphedema therapist may not have a good knowledge of billing practices. For example, they may not know how to verify copays, deductibles, prior authorization & pre-certifications or when to apply modifiers to HCPCS billing codes.
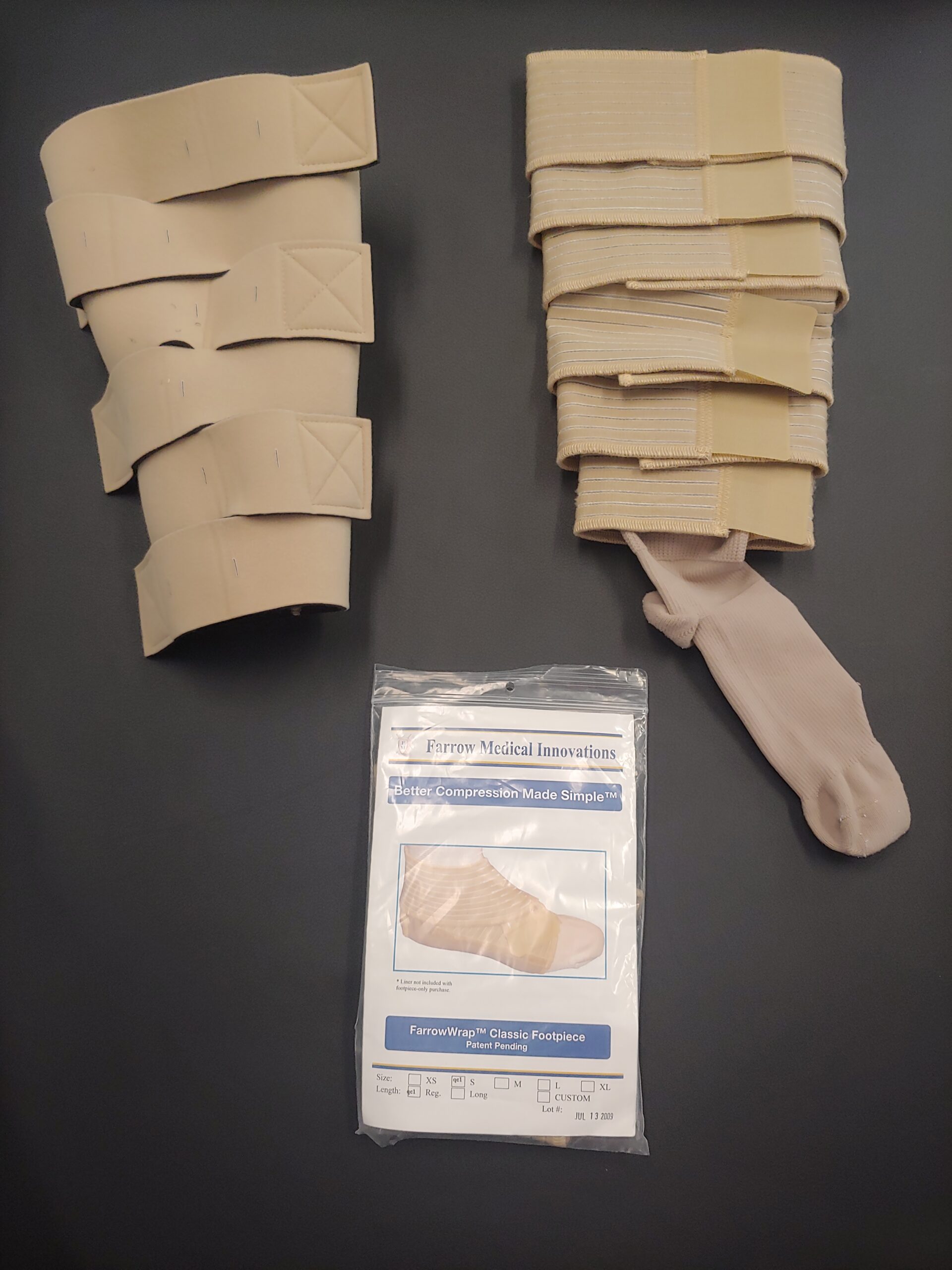
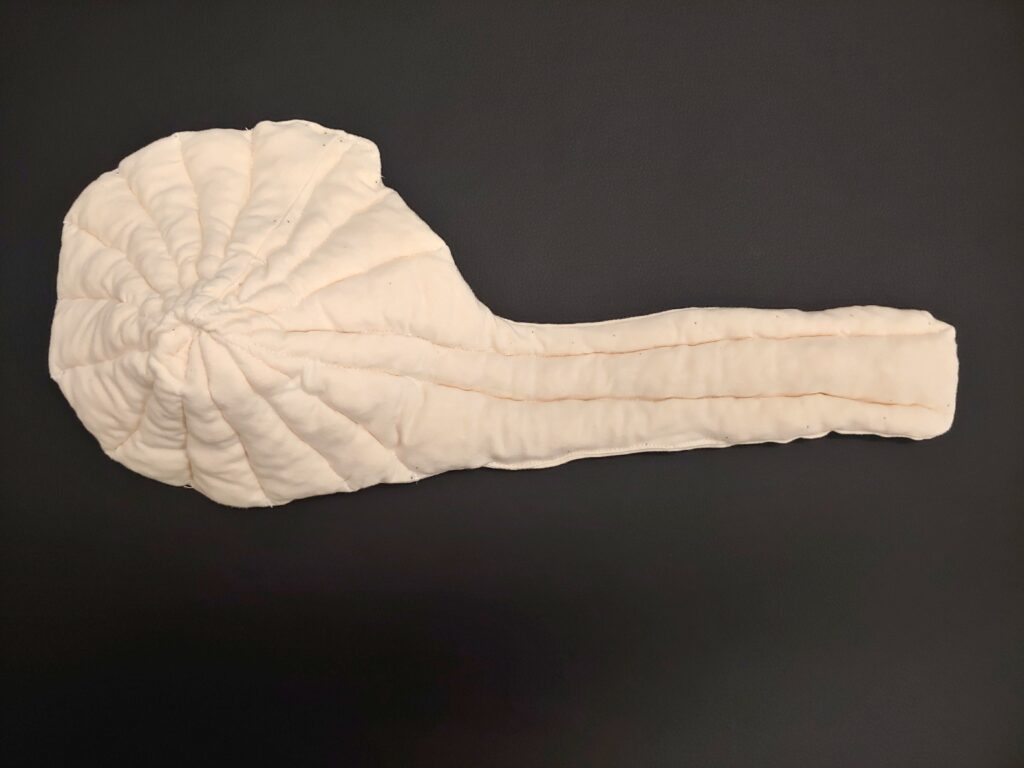
Thuasne chipped foam, Velcro lower leg garment. (Typically, a nighttime garment.)
DME fitters
Ideally, a DME fitter would be an experienced lymphedema therapist familiar with (& practiced in) fitting compression – including custom. They would also have a working knowledge of billing practices.
In cases where the DME fitter is not an experienced therapist, the next best scenario would be for the fitter to work closely with a lymphedema therapist. As noted above, unfortunately, many therapists don’t have a comprehensive knowledge of compression products. Their specialty is treating lymphedema. Hopefully, lymphedema training schools will add more compression training to their curriculum. But until then, most manufacturers offer free educational classes. A therapist only needs to contact them. Well-known manufacturers of lymphedema compression include:
- Lohmann Rauscher (includes Solaris)
- Essity (formerly BSN Medical – includes Jobst, Farrow, & JoViPak)
- Juzo
- Sigvaris (including Biacare)
- Medi
- Thuasne
- LympheDIVAs

LympheDIVAs readymade sleeve & glove
For therapists who want to be fitters
From my experience, I’d recommend a therapist who wants to fit compression start by learning one manufacturer’s products well. Lohman Rauscher, for example, offers both treatment supplies & compression garments. They would be a good manufacturer to start with. Once that manufacturer’s products are mastered, another manufacturer such as Essity (BSN Medical) could be learned. And so on.
Conclusion
The good news is compression garments & supplies will now be covered by Medicare. The bad news is lymphedema is a specialty field. Compression garments (& fitting them) are a niche within that specialty which many people do not have a good working knowledge of.
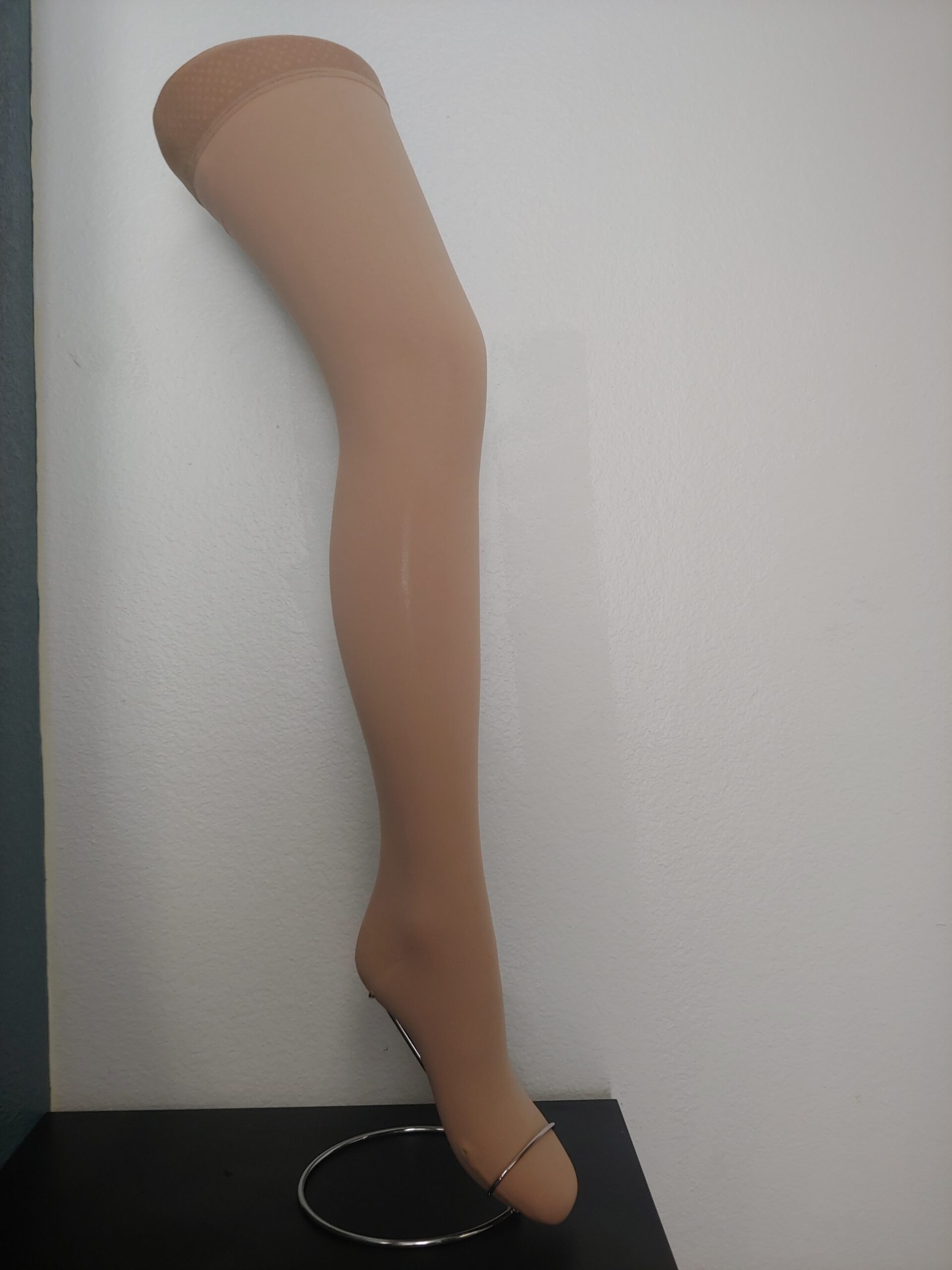
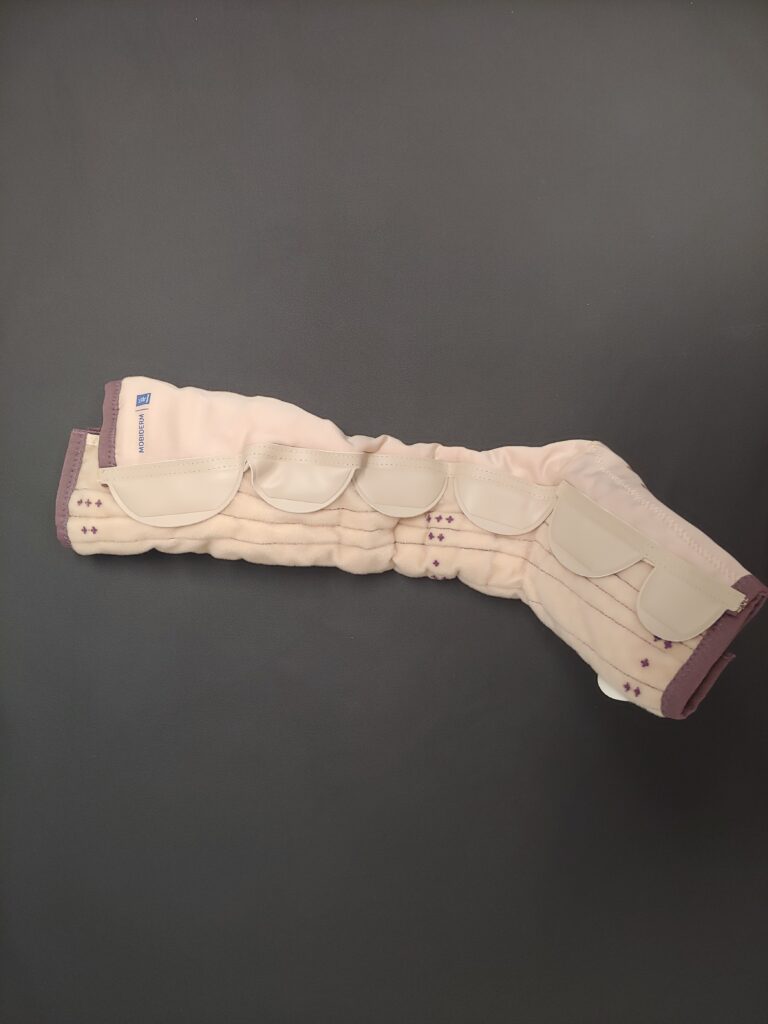
Jobst Readymade nighttime leg garment
P.S. If you don’t have traditional Medicare…
The Lymphedema Treatment Act team has requested you contact your insurance company (if it’s not traditional Medicare as your primary insurance) & request the company modify their coverage of lymphedema compression coverage (following Medicare’s new policy). If you have private insurance plans (whether employer-based or purchased separately), supplemental and secondary plans, Medicare Advantage, Medicaid, TriCare, & VA health care, the LTA team provides a template you can print here.

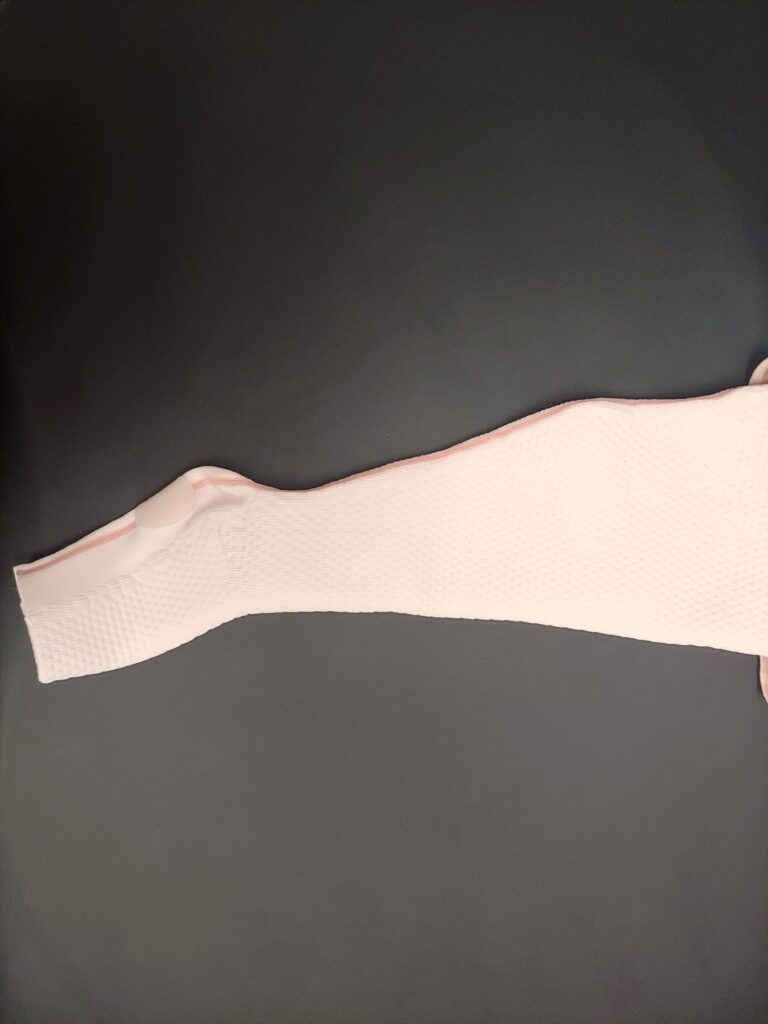
Juzo readymade sleeve