One word no one wants to hear is “cancer.” And when the diagnosis is given, a million thoughts run through a person’s mind. “Am I going to die?” “Will I lose my hair?” “Will I lose my breast?” As if the questions aren’t enough, the bombardment of medical terms and doctor specialties may ensue.
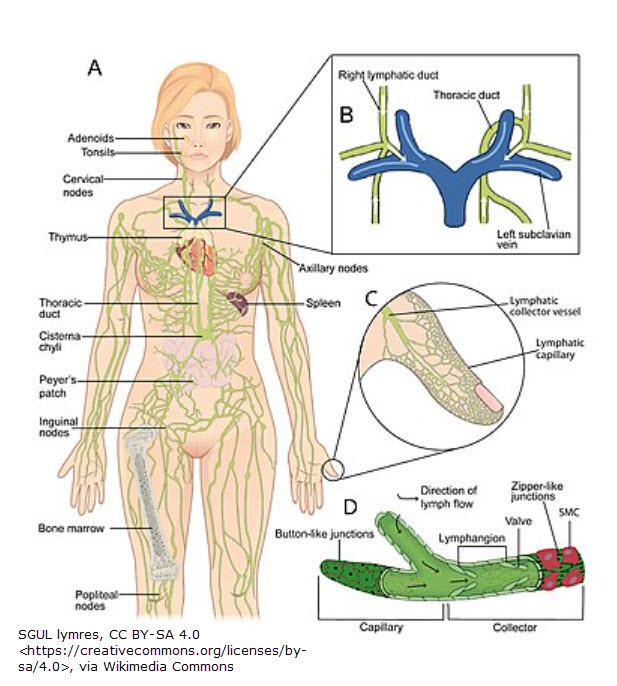
What’s lymphedema got to do with it?
In this early stage, the thought of potential lymphedema development is not a high priority (if it’s even discussed at all).
I’ve heard many stories from patients who were not told about the potential risk of developing lymphedema after lymph node removal and/or radiation. At a minimum, anyone going through cancer who has a lymph node removed and/or radiation should at least be given a handout on the signs and symptoms of lymphedema, what it is and what to do if signs and symptoms appear. Being given education about cellulitis and receiving baseline limb measurements would be an added benefit.
Photo by Pexels / Anna Tarazevich
How to recognize lymphedema onset
If you’ve been diagnosed with cancer, and you’ve had one or more lymph nodes removed (and/or radiation), you are at risk for developing lymphedema. How do you recognize this swelling condition? Here are signs and symptoms of lymphedema development according to stage:
- stage 0 (latency): no visible swelling but the involved area may feel heavy or achy
- stage I (reversible): protein begins to accumulate, visible swelling is present, elevation reduces swelling
- stage II (spontaneously irreversible): fibrosis (firmness) develops, pitting becomes more difficult, cellulitis infection may occur
- stage III (elephantiasis): tissue no longer indents (non-pitting) & becomes more firm, skin changes occur (hyperkeratosis, papillomas), lobules form, cellulitis infections may be common
Next month, we’ll look at recommendations to prevent lymphedema. Is there any science behind those recommendations?