Compression pumps may be known by different names. For example, “pneumatic compression pumps” or in a hospital setting, you may have heard the term “SCD” (sequential compression device). One refers to a type of pump while the other refers to the mode of compression delivery. This blog will overview the different types of pumps as well as their mode of delivery.
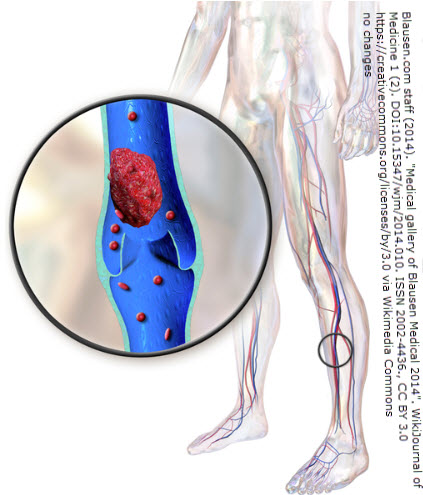
Pumps (in the medical sense) are devices advertised to improve blood and lymph circulation. More specifically, they may be used to prevent blood clots (such as after surgery), support wound healing, reduce post-operative swelling, or improve edema from venous insufficiency. But there are several differences among pumps. And not all pumps are appropriate for all conditions. When it comes to lymphedema, the wrong pump has potential to do more harm than good.
Types of Compression Pumps
- Pneumatic
- Pneumatic compression pumps use air pressure to apply external compression to limbs or other body parts. They’re composed of a sleeve which is placed around a limb. An external air pump inflates an air chamber (sometimes there is more than one air chamber) to provide compression. This can occur all at once, or when there are multiple chambers, it can be in a specific sequence (see also “Mode of Delivery” below).
- Regarding sequence, the inflation pattern may vary depending on the device (e.g. sequential vs. simultaneous inflation). Most are available in programmable models with adjustable settings and cycles. Some include a trunk component (e.g. Flexitouch, LymphaPress, Biocompression) to decongest first before moving to the swollen extremity (as we do in manual lymph drainage). These are used while seated or lying down. Duration is typically 45 minutes to an hour each day (sometimes twice per day depending on your doctor’s recommendation).
- Compression can be administered in an intermittent manner (compression is delivered at intervals or cycles, mimicking muscle contractions) or in a gradient (applying compression in a gradually reducing manner, with higher pressures distally & lower pressures proximally). When intermittent, there’s an inflation phase (i.e. “muscle contraction” pushing blood or fluid upward or proximally) followed by a deflation phase (i.e. “muscle relaxation” allowing refilling). Even this has variances: For example, some pumps have cycles allowing distal chambers to relax while a proximal chamber contracts (this can cause backflow). Other pumps or cycles maintain distal compression while the next chamber contracts.
Models:
1. single-chamber pumps – the entire sleeve inflates and deflates as one unit
2. sequential pumps – chambers inflate in a sequence from distal to proximal
3. advanced gradient pumps – chambers inflate sequentially and stay inflated until the cycle ends to prevent fluid backflow.
Examples of Devices:
- SCDs (Sequential Compression Devices)
- AIROS 6 and 8
- Flexitouch
- Lympha Press
- Biocompression 3004

Bio Compression Systems, Inc.
2. Non-pneumatic
The next type of compression is non-pneumatic. We’ll pick up that topic next month (with a company located right here in the Dallas, Tx area).