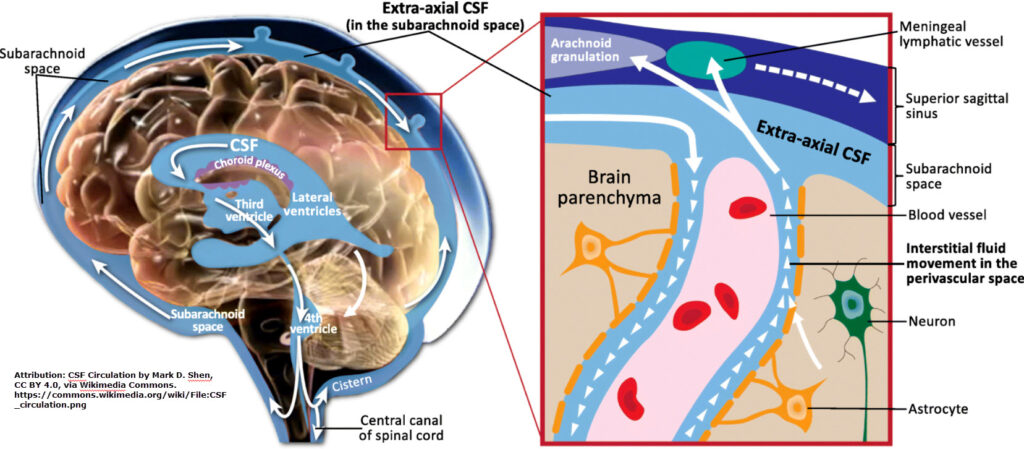
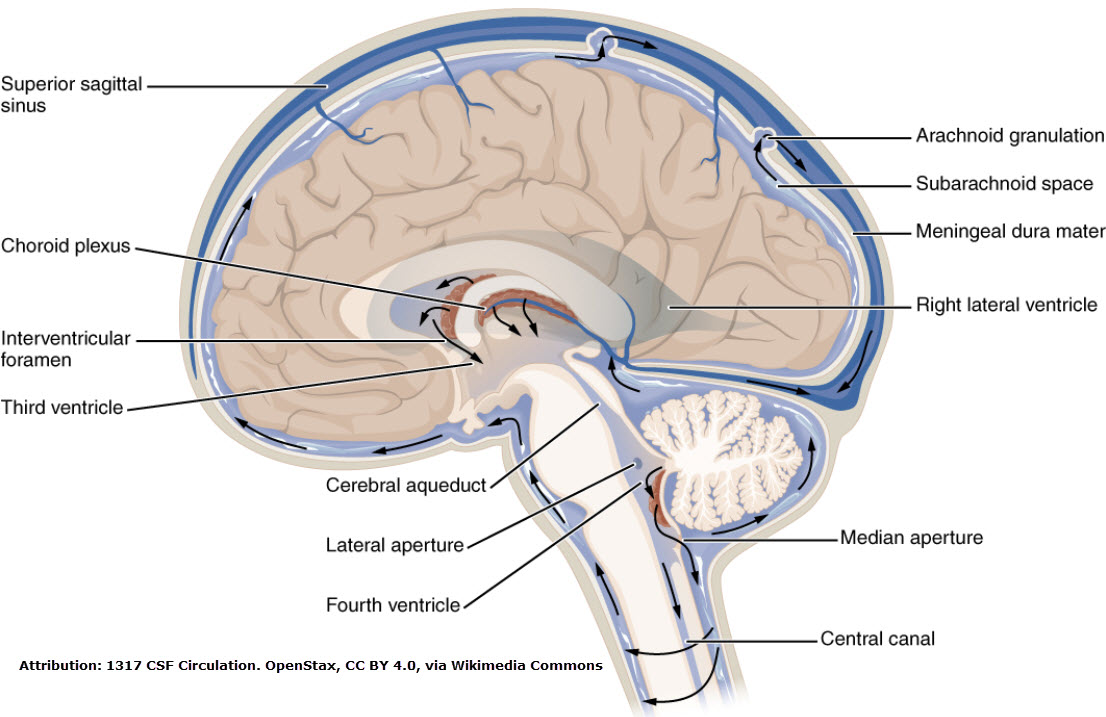
Last month we learned the brain has lymphatic vessels in the outer meningeal layer (the dura mater). Fluid inside the brain (cerebral spinal fluid) mixes with interstitial fluid in the innermost meningeal layer (the pia mater) before draining to the outer dura mater & its lymphatic vessels. When things go awry, dementia enters the picture. How does this occur?
The Glymphatic System
Along the blood vessels in the brain are cells called astrocytes. Astrocytes are a type of glial cell (a specialized WBC that are helpers or support cells for neurons & coat neurons with myelin).1 They come from monocytes & reside in the CNS.
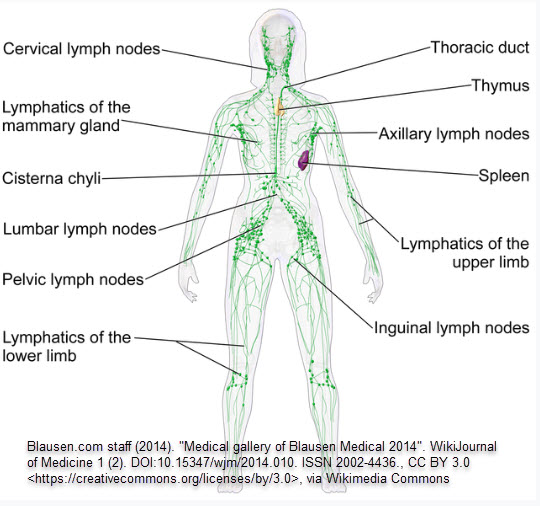
Astrocytes & microglial cells (another type of glial cell in the CNS) aid in nutrition, but they also help with immunity, waste clearance & maintaining homeostasis (just like the lymph system does). The perivascular channels containing these cells were named the “glymphatic system” because of their similarity to lymphatic system function.2,3,4
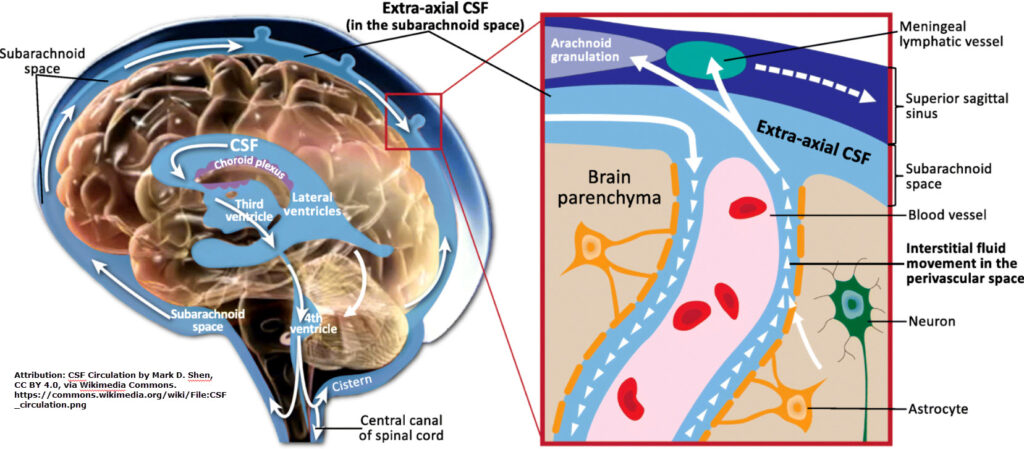
perivascular channels
The Cause of Dementia & Other Neurological Conditions
Previously, amyloid plaques were thought to be the cause of Alzheimer’s. Instead, they’re likely a by-product of the glymphatic system drainage disruption. More recent research is finding impairment in the glymphatic drainage is the likely cause of many neurological conditions, including dementia & Alzheimer’s (a form of dementia), by allowing a buildup of harmful waste to occur in the brain. There seem to be two primary culprits.
The Culprits
One culprit is faulty clearance of the fibrillar form of the beta-amyloid protein (an imbalance in the production & clearing of the peptide that comes from the processed amyloid protein, in particular).5,6 Another culprit is faulty clearance of the phosphorylated tau protein.7,8
The Stars of the CNS
Glial cells found in the brain (astrocytes, oligodendrocytes & microglia) can be considered the stars of the CNS because of their important role in preventing inflammation & their job of coating neurons with myelin.9 Myelin is the fatty sheath that surrounds & protects nerve fibers. It allows nerve impulses to travel quickly & efficiently.
diagram showing myelin sheath
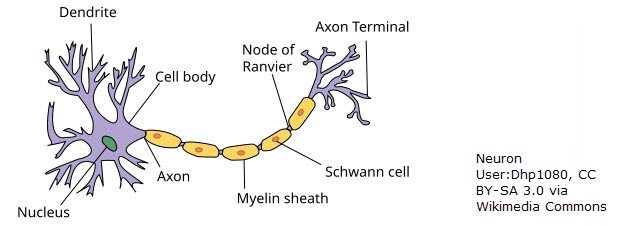
Brain inflammation (such as faulty clearance of substances mentioned above) causes this myelin sheath to break down, leading to the symptoms experienced in neurological diseases.10 How could MLD help? Find out in part 3.
References
1 https://my.clevelandclinic.org/health/body/23273-autonomic-nervous-system
2 https://www.nih.gov/news-events/nih-research-matters/new-brain-cleaning-system-discovered
3 https://www.researchgate.net/figure/Outline-of-the-glymphatic-system-This-figure-illustrates-that-perivascular-clearance_fig1_322688508
4 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4636982/#:~:text=The%20glymphatic%20system%20is%20a,from%20the%20
central%20nervous%20system
5 https://www.medicalnewstoday.com/articles/if-amyloid-accumulation-is-part-of-normal-aging-what-causes-alzheimers#:~:text=The%20researchers%20showed%20that%20the,journal%20of%20the%20Alzheimer’s%20Association
6 https://www.ncbi.nlm.nih.gov/books/NBK459119/
7 Garland EF, Hartnell IJ, Boche D. Microglia and Astrocyte Function and Communication: What Do We Know in Humans?. Front Neurosci. 2022;16:824888. Published 2022 Feb 16. doi:10.3389/fnins.2022.824888 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8888691/)
8 https://www.nih.gov/news-events/nih-research-matters/lymphatic-vessels-discovered-central-nervous-system#:~:text=The%20lymphatic%20system%20carries%20white,was%20termed%20the%20glymphatic%20system
9 https://my.clevelandclinic.org/health/body/23273-autonomic-nervous-system
10 https://my.clevelandclinic.org/health/body/22974-myelin-sheath
***EARLY VOTING TEXAS***
(DALLAS-FORT WORTH METROPLEX)